
WHAT IS W SITTING?

W sitting is a sitting position where a child’s legs form a “W.”. The child’s bottom is on the floor and their legs are turned out to the side.
WHY DO CHILDREN W SIT?
There are a few different reasons as to why a child may choose to sit in this position. It could be due to:
- Weakness in their hips
- Pre-existing orthopedic conditions
- Joint laxity (loose joints)
- Limitations in postural control such as core weakness leading to balance deficits in a seated position
Comfortability due to femoral anteversion (the position of the femur in the hip socket)- At birth, there is approximately 30-40 degrees of femoral anteversion. As a child ages the angle decreases to approximately 8-14 degrees in adults. (Luijkx, 2020)
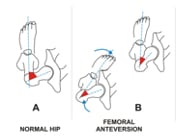
- This preference for internal rotation of the hip can lead to difficulty maintaining a cross-legged (criss cross applesauce) sitting position.
- At birth, there is approximately 30-40 degrees of femoral anteversion. As a child ages the angle decreases to approximately 8-14 degrees in adults. (Luijkx, 2020)
HOW CAN YOU CORRECT THE POSITION?
The number one way to correct W sitting position is to encourage alternative sitting positions. If you notice your child W sitting, use verbal cues to tell them to reposition their legs (for example: “criss cross applesauce” or “legs in front”), demonstrate new sitting positions and allow them to copy you, or physically reposition their legs into a new position. Motivate them to remain in this position with the use of toys or other fun activities. Below are some examples of alternative sitting positions to try with your child. Do not limit your attempts to just one position. Try a variety of them and see what works best for your child.
- Cross legged or criss cross applesauce

- This position places the legs in the exact opposite position of W sitting by allowing the hips to rotate outwards instead of in. This position also promotes better posture and allows for reaching across midline to play and explore more of their environment.
- Side sit

- This position allows for a transition between W sitting and criss cross sitting. It promotes more need for postural stability and allows rotation to reach across the midline.
- If you are attempting this position, be sure to switch sides, to allow for external rotation of each hip.
- Butterfly sit

- This position allows for a deeper stretch to the muscles of the hip than the aforementioned criss cross position. Encourage your child to keep their knees close to the ground to provide as much stretch as possible.
- Long sit

- This position allows for the legs to be in a more neutral position and can help provide a stretch to the child’s hamstrings.
- Tall kneel

- This position aligns the hips in neutral, but also requires more postural control to strengthen the hips and the trunk during play. For more advanced children, have your child try “walking” on their knees in this position to collect their toys, puzzle pieces, or other motivating objects.
Aside from various sitting positions, it is also important to encourage your child to play on their tummy. Having them lay on their stomach allows for a hip stretch and provides a different viewpoint for exploration and play. With the consistent implementation of these new sitting positions, you should see a decrease in their preference for W sitting, an improvement in posture, and overall improvements in their alignment.
WHEN SHOULD YOU BE CONCERNED?
Although many children W sit and a large number of them “out-grow” it without any functional or physiological issues, there are a few negative effects that may require an evaluation for intervention.
- Frequent falls or trips
- A higher falling frequency has been noted in individuals with femoral anteversion. Those children with femoral anteversion fell four times more often during running and three times more often during fast walking than their healthy peers. (Leblebici et al., 2019)
- Reports of pain or discomfort in the child’s hips or legs
- If you notice your child cries and points at their hips, knees, ankle, or feet, they may be in pain due to an abnormal alignment of their legs.
- Delayed development of gross motor skills (Leblebici et al., 2019)
- Watch how your child plays with peers their age. You may be able to see discrepancies in their abilities that could be a cause of concern.
- For example: Children should be able to jump forward approximately four inches by the time they are two years old. If they are not completing this task and you watch other children their age playing at the playground jumping around, this may be a signal of some gross motor delay.
- Abnormalities with gait (such as in-toeing, “pigeon-toed,” while walking)
- In-toeing was detected in approximately 6% of children who preferred W sitting (Altinel et al., 2007). In-toeing may be due to femoral anteversion as mentioned above, tibial torsion (a rotation of the lower leg bones), or abnormalities of the position of the feet.
- Another abnormality associated with W sitting is flat feet which may lead to further orthopedic issues as the child ages (Chen et al., 2010)
- Difficulty achieving seated positions other than W sitting
- If you are attempting the alternative positions, and your child is unable to obtain or maintain the positions, that may indicate tightness in the joints.
- Fatigue after short periods of activity
- During prolonged walking (for example: grocery shopping, walking at the mall), children with femoral anteversion showed rapid onset of fatigue as compared to their healthy counterparts. (Leblebici et al., 2019)
If you continue to struggle with W sitting, or find that despite these strategies, any of the above listed concerns arise, consider seeking support from a trusted therapist. A skilled pediatric physical therapist will be able to evaluate your child to further investigate range of motion, strength, alignment, gait pattern, and overall gross motor development. They can provide exercises and various activities or interventions that are used to improve these categories if an issue is noted. The physical therapist would also be able to make a recommendation if further specialists need to be involved. At Carolina Pediatric Therapy, we have a team of physical therapists who are prepared to walk beside you on your journey.
REFERENCE LIST
- Luijkx, T., 2020. Femoral Anteversion | Radiology Reference Article | Radiopaedia.Org. [online] Radiopaedia.org. Available at: radiopaedia.org.
- Leblebici, G., Akalan, E., Apti, A., Kuchimov, S., Kurt, A., Onerge, K., Temelli, Y. and Miller, F., 2019. Increased femoral anteversion-related biomechanical abnormalities: lower extremity function, falling frequencies, and fatigue. Gait & Posture, 70, pp.336-340.
- Altinel, L., Köse, K. C., Aksoy, Y., Işik, C., Erğan, V., & Ozdemir, A. (2007). Hip rotation degrees, intoeing problem, and sitting habits in nursery school children: An analysis of 1,134 cases. Acta Orthopaedica Et Traumatologica Turcica, 41(3), 190.
- Chen, K., Yeh, C., Tung, L., Yang, J., Yang, S. and Wang, C., 2010. Relevant factors influencing flatfoot in preschool-aged children. European Journal of Pediatrics, 170(7), pp.931-936.
Leilani Maybin, PT, DPT is a is a Licensed Physical Therapist with Carolina Pediatric Therapy. She is a part of an interprofessional collaborative team including behavioral health, occupational therapists, physical therapists, speech-language pathologists, and psychologists dedicated to supporting and promoting children’s development and well being.
Click on the button below to download the article:

Want to know how a Therapist can Help?
Call (828) 398 0043 or click on the schedule button.

